Leveraging Digital Health Technologies To Strengthen The Fight Against Tuberculosis (TB) In Malawi
This is the 13th post in a blog series to be published in 2022 by the Secretariat on behalf of the AU High-Level Panel on Emerging Technologies (APET) and the Calestous Juma Executive Dialogues (CJED)
Tuberculosis (TB) is the world's ninth leading cause of mortality. This disease is one of the top causes of death in Africa and surpasses human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS). Notably, the African continent has reported that TB has infected more than a quarter of all TB fatalities across the world. Furthermore, the upsurge of multidrug-resistant tuberculosis (MDR-TB) has posed a severe health hazard.[1] Thus, putting the advances that have been made against TB at significant risk. Regrettably, Africa has 16 of the world's 30 countries experiencing the highest TB burden.[2]
To address these TB-related infection challenges, the Heads of States and Governments of African countries established the Catalytic Framework to combat and eradicate TB infection cases and deaths in Africa by 2030. Besides the Catalytic Framework to eliminate TB, Malaria, and HIV/AIDS by 2030, the African Union Agenda 2063 and the United Nation’s Sustainable Development Goals (SDGs) are also providing strategic methodologies to hasten efforts toward eradicating TB and enhance healthcare systems.[3]
Furthermore, the Southern Africa Tuberculosis and Health Systems Support (SATBHSS) regional project was launched in 2016 so to strengthen the response of the healthcare sector to TB and occupational lung diseases.[4] This project is being implemented in four (4) Southern African Development Community (SADC) Member States, namely, Lesotho, Malawi, Mozambique, and Zambia. The African Union Development Agency – NEPAD (AUDA-NEPAD) and East, Central and Southern Africa Health Community (ECSA-HC) are collaborating to offer technical support in the project implementation of the participating SADC countries.[5] Among other outputs, this project improved the coverage and quality of TB control and occupational lung disease services, strengthened the regional capacity to manage the burden of TB and occupational lung diseases, and strengthened the country-level and cross-border preparedness and response to disease outbreaks.
However, despite these efforts, several African countries have fallen short of accomplishing these goals of ending the TB infections as aspired in these frameworks. Notably, poverty, inequality, and limited healthcare infrastructure have inhibited the capacity of many African countries to attain universal health coverage. Some African countries have even failed to respond to communicable diseases such as TB effectively.
Notably, TB has remained a major public health challenge for African countries such as Malawi. The World Health Organisation reported that in 2020, Malawi recorded approximately 27 000 TB cases, and 4200 of those cases were children.[6] Furthermore, the TB-related mortality death rate was approximately 1400 during the same period. Additionally, TB infections and deaths have been recorded among people infected with HIV/AIDS. For example, the TB infection rate has been reportedly 6 in every 10 people with people infected with HIV. Thus, TB is one of the priority diseases within Malawi’s Essential Health Package (EHP).[7]
The prevention and treatment of TB in Malawi, like in many other African countries, have continued to confront some challenges. These challenges include the late diagnosis of potential TB patients, limited patient adherence to daily TB medication because of the pill burden, and complex delivery modes of medication. Additionally, there are challenges of inadequate financing and prolonged travel time to healthcare facilities, especially in rural Africa. In Malawi, the latter challenge is compounded by the over 50% population that resides outside the recommended 5 km perimeter from nearby healthcare facilities.[8]
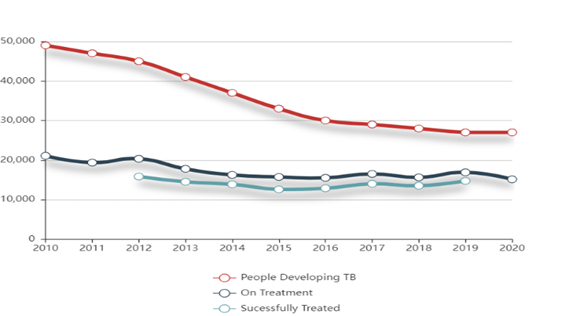
Figure 1. The number of people developing TB on treatment and successfully treated in Malawi between 2010 – 2020. Source: https://www.stoptb.org/static_pages/MWI_Dashboard.html.
Presently, the TB treatment regimens and strategies such as the in-person directly observed therapy have been progressively declining the TB infection rates per year (Figure 1). However, this approach has been described as costly and logistically challenging to administer. This is because the TB programme staff should physically observe the patients to ensure that they ingest the medication in locations that are convenient to the patients.[9] Furthermore, to strengthen the appropriate management of TB, there should be a systematic screening of TB patients among high-risk groups such as older people and those previously treated for TB. However, approximately 29% of new TB cases are unidentifiable, and in some cases, healthcare centres fail to notify the patients officially.[10] This is partly due to the failure of Malawi’s healthcare system to actively diagnose TB patients because of the remoteness and inadequate healthcare centres. However, even though most TB deaths are preventable, if detected and treated at an early stage, TB still causes significant deaths in Malawi, as well as other African countries.[11]
To accomplish the better management systems for TB, the African Union High Level Panel on Emerging Technologies (APET) is challenging African countries to consider digital health technologies for the care and control of TB. Digital health technologies can be utilised to promote patient healthcare and enable electronic directly observed therapy (eDOT).[12] This can focus primarily on TB screening, diagnosis, and treatment adherence. Primarily, the eDOT focuses on administering, managing, and supporting TB patients to enhance adherence and ensure regular intake of TB medicines. This can also help manage patients in their homes instead of frequent clinic visits.[13]
There has been limited evidence that digital health technologies can enhance TB care. However, more studies of better quality should be undertaken to determine how these technologies can enhance the TB care programme performance.[14] However, APET believes that given the circumstances and challenges of the African continent, digital technologies can be utilised to support TB treatment adherence and treatment protocols. This is because digital technologies are changing healthcare delivery globally, as witnessed by the dramatic growth in such areas as electronic health records, telehealth for “virtual” patient encounters, and teleradiology for remote interpretation of imaging studies.
Digital health technologies can be utilised for surveillance and monitoring to enable health information system management.[15] These systems can be utilised to assess and evaluate the burden of TB disease and death and further monitor drug resistance. It is also important to enhance the TB drugs management programme to enable drug stock management systems, standards development, and training programmes. Most importantly, digital health technologies can enable e-learning using digital media and devices to enhance access to guidance, consultation, and interaction.[16]
APET is recommending that African countries such as Malawi should augment existing treatment regimes with digital health technologies such as short message services (SMS) and smartphone applications to accomplish better TB management systems. Smartphone applications can best manage infectious disease management irrespective of geographical barriers.[17] For example, the National TB Control Programme in Malawi, in collaboration with international partners, after noticing the limited adherence of TB patients to medication which had resulted in significant relapses, developed the Frontline SMS:Medic as a medicine reminder application. This application was developed to enhance adherence to medication in TB patients.
As a case in point, the Namitete Hospital undertook the piloting phase of the Frontline SMS:Medic project in 2009. Within the first five (5) months of its operation, the Frontline SMS:Medic campaign demonstrated significant impact as it enabled hospitals to double their treatment and management capacity of patients.[18]
Furthermore, the Frontline SMS:Medic also enabled hospitals to prescribe medication and dosage use. This system enabled the auxiliary health workers to “google” the drug names. In response, the application can automatically respond with information on the dosages and usage of TB drugs. Consequently, this enables healthcare workers to provide and obtain patient status updates. Furthermore, healthcare workers can make follow-up calls for further medical consultations and treatment.[19]
Predominantly, Malawi utilises paper-based medical record-keeping, which has been observed to inhibit easier access to patient records and tracking. In 2001, the Malawian Government introduced the electronic medical record system (EMRS).[20] Consequently, the EMRS addresses the frequent data losses. This is because a majority of patients' hard copy booklets containing their health history can easily be lost through wear and tear. Fundamentally, the EMRS system improved the patient management protocols, enhanced the integration of TB and HIV healthcare services, and enriched healthcare decision-making.
Furthermore, the EMRS platform was expanded from servicing 19 healthcare facilities in 2012 to 50 healthcare facilities across Malawi in 2021.[21] Notably, as the EMRS is expanding across the country, the system's capabilities are also evolving in response to the progressively growing national information demands. The EMRS platform has incorporated malaria and diabetes records, among other ailments.
In following the progressive successes that have been observed in Malawi, APET recognises that the African continent can significantly benefit from adopting digital health technologies to monitor and manage their TB patients. However, to expand the impact and expedite the adoption of these digital health technologies, APET is challenging African countries to enhance investments in digital health technology-related infrastructure. APET appreciates that African countries are steadily and progressively developing effective TB prevention and treatment techniques, as exhibited by the considerable decline in TB infection and death cases across the African continent. However, the effects are currently not widespread. Thus, APET suggests that to complement the progressive successes, African countries should adopt digital health technologies. Thus, if these technologies can be adopted in their entirety, African countries can effectively eliminate TB cases in a coordinated manner.
Featured Bloggers – APET Secretariat
Justina Dugbazah
Barbara Glover
Bhekani Mbuli
Chifundo Kungade
[1] https://www.afro.who.int/news/tuberculosis.
[2] https://www.stoptb.org/news/heads-of-state-pledge-support-successful-un-high-level-meeting-tb-during-africa-union-summit.
[3] https://au.int/sites/default/files/newsevents/workingdocuments/27513-wd-sa16949_e_catalytic_framework.pdf.
[4] Improving Cross-Border disease surveillance in Malawi and Mozambique. https://www.satbhss.org/malawi/media-center/news-information/improving-cross-border-disease-surveillance-malawi-and.
[5] SOUTHERN AFRICA TB AND HEALTH SYSTEMS SUPPORT PROJECT. SATBHSS Annual Report 2020. https://www.satbhss.org/malawi/media-center/news-information/ministry-health-senior-management-team-visits-satbhssp-impact.
[6] https://www.stoptb.org/static_pages/MWI_Dashboard.html.
[7] Kirolos, A., Thindwa, D., Khundi, M., Burke, R. M., Henrion, M., Nakamura, I., Divala, T. H., Nliwasa, M., Corbett, E. L., & MacPherson, P. (2021). Tuberculosis case notifications in Malawi have strong seasonal and weather-related trends. Scientific reports, 11(1), 4621. https://doi.org/10.1038/s41598-021-84124-w.
[8] Kim, E. T., Singh, K., Speizer, I. S., Angeles, G., & Weiss, W. (2019). Availability of health facilities and utilization of maternal and newborn postnatal care in rural Malawi. BMC pregnancy and childbirth, 19(1), 503. https://doi.org/10.1186/s12884-019-2534-x.
[9] https://stoptb.org/assets/documents/resources/publications/acsm/mHealth%20to%20Improve%20TB%20Care.pdf.
[10] Laghari, M., Sulaiman, S., Khan, A. H., Talpur, B. A., Bhatti, Z., & Memon, N. (2019). Contact screening and risk factors for TB among the household contact of children with active TB: a way to find source case and new TB cases. BMC public health, 19(1), 1274. https://doi.org/10.1186/s12889-019-7597-0.
[11] https://www.afro.who.int/health-topics/tuberculosis-tb.
[12] Burzynski, J., Mangan, J. M., Lam, C. K., Macaraig, M., Salerno, M. M., deCastro, B. R., Goswami, N. D., Lin, C. Y., Schluger, N. W., Vernon, A., & eDOT Study Team (2022). In-Person vs Electronic Directly Observed Therapy for Tuberculosis Treatment Adherence: A Randomized Noninferiority Trial. JAMA network open, 5(1), e2144210. https://doi.org/10.1001/jamanetworkopen.2021.44210.
[13] Munro, S. A., Lewin, S. A., Smith, H. J., Engel, M. E., Fretheim, A., & Volmink, J. (2007). Patient adherence to tuberculosis treatment: a systematic review of qualitative research. PLoS medicine, 4(7), e238. https://doi.org/10.1371/journal.pmed.0040238.
[14] Ngwatu, B. K., Nsengiyumva, N. P., Oxlade, O., Mappin-Kasirer, B., Nguyen, N. L., Jaramillo, E., Falzon, D., Schwartzman, K., & Collaborative group on the impact of digital technologies on TB (2018). The impact of digital health technologies on tuberculosis treatment: a systematic review. The European respiratory journal, 51(1), 1701596. https://doi.org/10.1183/13993003.01596-2017.
[15] Budd, J., Miller, B.S., Manning, E.M. et al. Digital technologies in the public-health response to COVID-19. Nat Med 26, 1183–1192 (2020). https://doi.org/10.1038/s41591-020-1011-4.
[16] Niranjan Konduri, Francis Aboagye-Nyame, David Mabirizi, Kim Hoppenworth, Mohammad Golam Kibria, Seydou Doumbia, Lucilo Williams, Greatjoy Mazibuko, Digital Health, Digital health technologies to support access to medicines and pharmaceutical services in the achievement of sustainable development goals, https://doi.org/10.1177/2055207618771407.
[17] https://www.frontiersin.org/articles/10.3389/fpubh.2021.653337/full .
[18] Nglazi, M. D., Bekker, L. G., Wood, R., Hussey, G. D., & Wiysonge, C. S. (2013). Mobile phone text messaging for promoting adherence to anti-tuberculosis treatment: a systematic review. BMC infectious diseases, 13, 566. https://doi.org/10.1186/1471-2334-13-566.
[19] https://www.theguardian.com/technology/2009/mar/27/mobile-phones-sms.
[20] Mkalira Msiska, K. E., Kumitawa, A., & Kumwenda, B. (2017). Factors affecting the utilisation of electronic medical records system in Malawian central hospitals. Malawi medical journal : the journal of Medical Association of Malawi, 29(3), 247–253. https://doi.org/10.4314/mmj.v29i3.4.
[21] Shiroya, V., Shawa, N., Matanje, B., Haloka, J., Safary, E., Nkhweliwa, C., Mueller, O., Phiri, S., Neuhann, F., & Deckert, A. (2021). Reorienting Primary Health Care Services for Non-Communicable Diseases: A Comparative Preparedness Assessment of Two Healthcare Networks in Malawi and Zambia. International journal of environmental research and public health, 18(9), 5044. https://doi.org/10.3390/ijerph18095044.


